During 2016 we will be periodically blogging about resources, like The Red Barn Equestrian Therapy, listed on the site. Each location has been personally visited and we have had an opportunity to spend time viewing the facility plus discussing the services available. Traumatic Brain Injury Resources wants to provide the visitors to the site with some first hand insight on a wide variety of the resources listed throughout the state of Alabama.The information shared with you will be our impressions of their facilities, services available and the personnel I have met at each location.
You will be always able to just click on any resource listed and contact them directly to determine if they fit your situation and current needs. However, by offering you our perspective, when conducting a resource visitation, the additional depth of knowledge may be helpful in your decision making process.
This site will continue to monitor and add new resources, whenever we are aware of their existence and encourage visitors to notify us of any service providers they feel should be included.
I recently visited The Red Barnmeeting with the founder, Joy O’Neal, who spent the greater part of the day touring me through the facility while explaining the unique approach of equestrian therapy. Individuals in need of therapeutic intervention are often difficult to reach through the standard therapy programs available. The Red Barnhas developed an equestrian therapy intervention program that breaks down those self imposed barriers. Here working one on one with a patient assisted by horses, allows them to introduce a series of training courses focused on improving their overall well being.
The Red Barnopened in 2009 with a profound faith in God’s Healing Hand to reach the injured through the utilization of equestrian therapy to lead them to a fuller and richer life while cooping with their afflictions. The approach here not only deals with the individual, but reaches out to encompass other family members to assist them in gaining a deeper understanding as to how they can effectively function as a total inclusive unit. This is reflected in the physical development of the 33 acres The Red Barn occupies and the staffs’ approach to every patient, analyzing his/her needs along with those of their family members.
As I toured the grounds, I was impressed with the degree of planning evidenced and the amount of development that had occurred to this property in a short period of time. It is evident that the personnel remains consistently focused on understanding the needs of patients and making the necessary adjustments to the facilities to meet those needs.
The Red Barn has a diverse stafffocused on creating programs designed to enrich the training experience of the individuals participating while enhancing their growth. The full time staff’s expertise is further supplemented by a caring community of volunteers providing a wealth of knowledge and skills acquired in their professional careers.
During my visit I met with one of those individuals,Wyspr Black a CHA IRD certified instructor with a master’s from Auburn University in Rehabilitation Counseling and Vocational Education. Her special interest in working with individual’s suffering from traumatic brain injuries combined with her love of horses since she was eight, makes her an ideal fit forThe Red Barn. Wyspr plays an instrumental role in developing and implementing equestrian therapy programs uniquely designed for Traumatic Brain Injury patients.
As evidenced in this photo,The Red Barn offers equestrian therapy and training for individuals with physical, cognitive and emotional disabilities teaching them life skills, which provide a solid foundation for developing a productive life. Depicted here is the initial teaching stall within the barn where a student begins to learn about the care and handling of a horse prior to meeting with a live animal. This organization offers an opportunity for individuals of all ages to explore and expand their horizons beyond the limitations experienced from Traumatic or Spinal Cord Injury.
The Red Barn has developed the following programs to serve this community’s needs:
THE RED BARN EQUESTRIAN THERAPY – SADDLE UP– Weekly riding lessons for those with physical, cognitive or emotional disabilities and special circumstances.
<
THE RED BARN EQUESTRIAN THERAPY – HORSE PLAY– Traditional day camps with art, music, outdoor education…and horses!
THE RED BARN EQUESTRIAN THERAPY – TAKE THE REINS – It is our honor and privilege to serve active or inactive military personnel. We offer a customized experience for each individual or group.
The Red Barnis a 501(c)3 agency relying on the contributions of the community to continue and expand the innovative work it does to develop effective rehabilitative programs for individuals with Traumatic Brain and Spinal Cord Injuries.
Neuronal cells may be repaired in the near future opening the potential to reverse brain damage, spinal cord injuries and the devastating effects of diseases such as MS, ALS, Parkinson’s, Dementia and Alzheimer. For the first time researchers have direct evidence that viruses can infect neuronal cells, raising hope that antiviral therapy might be effective against neurologic diseases and cell damage, according to a new study.
A neurological disorder is any disorder of the body nervous system. Structural, biochemical or electrical abnormalities in the brain, spinal cord or other nerves can result in a range of symptoms. Examples of symptoms include paralysis, muscle weakness, poor coordination, loss of mental control, sensation, seizures, confusion, pain and altered levels of consciousness
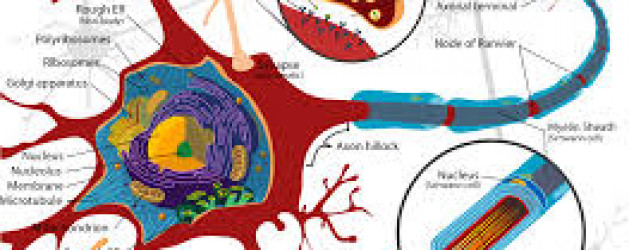
Neurons are nerve cells that transmit nerve signals to and from the brain at up to 200 mph. The neuron consists of a cell body (or soma) with branching dendrites (signal receivers) and a projection called an axon, which conduct the nerve signal. At the other end of the axon, the axon terminals transmit the electro-chemical signal across a synapse (the gap between the axon terminal and the receiving cell). The word “neuron” was coined by the German scientist Heinrich Wilhelm Gottfried von Waldeyer-Hartz in 1891 (he also coined the term “chromosome”).
There are different types of neuronal cells. They all carry electro-chemical nerve signals, but differ in structure (the number of processes, or axons, emanating from the cell body) and are found in different parts of the body.
Sensory neurons or Bipolar neurons carry messages from the body’s sense receptors (eyes, ears, etc.) to the CNS. These neurons have two processes. Sensory neuron account for 0.9% of all neurons. (Examples are retinal cells, olfactory epithelium cells.)
Motoneurons or Multipolar neurons carry signals from the CNS to the muscles and glands. These neurons have many processes originating from the cell body. Motoneurons account for 9% of all neurons. (Examples are spinal motor neurons, pyramidal neurons, Purkinje cells.)
Interneurons or Pseudopolare (Spelling) cells form all the neural wiring within the CNS. These have two axons (instead of an axon and a dendrite). One axon communicates with the spinal cord; one with either the skin or muscle. These neurons have two processes. (Examples are dorsal root ganglia cells.)
The core component of the nervous system in general, and the brain in particular, is the neuron or nerve cell, the “brain cells” of popular language. A neuron is an electrically excitable cell that processes and transmits information by electro-chemical signalling. Unlike other cells, neurons never divide, and neither do they die off to be replaced by new ones. By the same token, they usually cannot be replaced after being lost, although there are a few exceptions.
Information transmission within the brain, such as takes place during the processes of memory encoding and retrieval, is achieved using a combination of chemicals and electricity. It is a very complex process involving a variety of interrelated steps, but a quick overview can be given here.
Unlike other body cells, most neurons in the human brain are only able to divide to make new cells (a process called neurogenesis) during fetal development and for a few months after birth.
These brain cells may increase in size until the age of about eighteen years, but they are essentially designed to last a lifetime.
During childhood, and particularly during adolescence, a process known as “synaptic pruning” occurs.
Although the brain continues to grow and develop, the overall number of neurons and synapses are reduced by up to 50%, removing unnecessary neuronal structures and allowing them to be replaced by more complex and efficient structures, more suited to the demands of adulthood.
The data demonstrate that Epstein Barr Virus (EBV) and Kaposi’s sarcoma–associated herpesvirus (KSHV) are able to effectively infect neuronal cell lines, as well as primary neurons. “This phenomenon may potentially provide clues to their contribution to the pathogenesis of human neural diseases,” stated the researchers, led by senior author Erle S. Robertson, PhD, of the University of Pennsylvania in Philadelphia, PA.
“In this study, for the first time, we have successfully demonstrated the in vitro infection of Sh-Sy5y (a human neuroblastoma cell line) and Ntera2 cells (a neuronally committed human teratocarcinoma cell line), as well as human primary neurons. We have also determined that the infection is predominately lytic. Additionally, we also report infection of neuronal cells by KSHV in vitro similar to that by EBV,” stated the authors.
They believe that these findings may “open new avenues of consideration related to neuronal pathologies and infection with these viruses. Furthermore, their contribution to chronic infection linked to neuronal disease will provide new clues to potential new therapies.”
In many debilitating neurodegenerative diseases, including MS, the efficiency of electrochemical signals is greatly reduced, they noted, often leading to problems related to cognition and muscular activity. “It is likely that viral infection with EBV or KSHV may severely reduce these signals, leading to reduced cognition and reduced neuromuscular function,” they stated.
The results clearly show that infection of neuronal cells can occur, but further studies are needed to understand the underlying mechanism of these infections and their relevance to neuronal diseases.
IT SOUNDS like the dark plot of a vampire movie – Young blood rejuvenates our cells. In October 2014, people with Alzheimer’s disease started to be injected with the blood of young people in the hope that it will reverse some of the damage caused by that condition. But holds promise for individuals suffering for a wide range issues that have impacted their body and effected the quality of their life style. Just imagine the implications of reversing Traumatic Brain Injuries, Parkinson’s, MS, ALS, Repairing Damaged Organs, Surgical Healing, Aging of Skin, Muscle and Vascular Development.
In the first human trial of the effects of young blood, at Stanford University, infusions of blood plasma from young people are being given to older people. The preliminary results have surprised the research team, since it appears that young blood rejuvenates all of the cells within the recipients’ bodies are showing marked improvement.
Blood Stanford Test
The scientists behind the experiment have evidence on their side that young blood rejuvenates. Work in animals has shown that a transfusion of young mouse blood can improve cognition and the health of several organs in older mice. It could even make those animals look younger. The ramifications for the cosmetics and pharmaceutical industries could be huge, if the same thing happens in people.
The study was published in Nature Medicine in 2014. Immediately, emails flooded in to Wyss-Coray’s inbox. Alzheimer’s patients wanted infusions of young blood. So did numerous aged billionaires interested in the potential that young blood rejuvenates. One, who flies around in a jet with his name emblazoned on the side, invited Wyss-Coray to an Oscars after-party this year. (He didn’t go.) Another correspondent wrote with a more disturbing offer: he said he could provide blood from children of whatever age the scientists required. Wyss-Coray was appalled. “That was creepy,” he said.
But it wasn’t until spring 2012 that plans to form a company emerged. Nikolich, an entrepreneur and neuroscientist at Stanford, had flown to Hong Kong to visit the family of Chen Din-hwa, a Chinese billionaire known as the King of Cotton Yarn. Three years earlier, Chen had died, aged 89, with Alzheimer’s disease. His grandson told Nikolich that towards the end of his life, Chen barely recognised his own family. Then he had a plasma transfusion for an unrelated condition, which seemed to have a spectacular effect. His mind was clearer and he was suddenly cogent. His grandson indicated that Alzheimer’s disease seem to historical effect the male of the family often at an early age.
Nikolich told them about Wyss-Coray’s research and the potential for plasma-based therapies that revitalised the ageing brain. Before long, the conversation turned to starting a company. The family invested a year later. The money got Alkahest established and ready to launch the first human trial of young plasma.
Alkahest’s ultimate goal – to identify the key proteins in plasma that rejuvenate or age human tissues and then manufacture a product that uses them – could take 10 to 15 years. In the near term, the company has another strategy. Earlier this year, the Spanish blood products firm, Grifols, pledged $37.5m for a 45% stake in Alkahest. With another $12.5m, the company will bankroll more research in exchange for rights to Alkahest’s first products. Over the next two years, Alkahest will take human plasma and divide it into fractions that are rich in different proteins. Each fraction will then be tested in mice to see if they boost brain function. Any that do will be swiftly introduced into human trials and developed into the first generation of products.
The Alkahest trial is small. Sha, a specialist in behavioral neurology, can enroll only 18 people aged 50 to 90 with mild to moderate Alzheimer’s disease. Each receives a unit of young human plasma or saline once a week for four weeks. They have the next six weeks off, then have four more weeks of infusions. Those who had plasma first time around get saline and vice versa. The process is blinded, so neither the patients, nor their carers, nor Sha herself, know who is receiving what. Throughout the trial, doctors will look for cognitive improvements. Only at the end of the trial, as soon as October this year, will Sha analyse the findings.
If patients improve with infusions of young plasma, scientists will be ecstatic. But the finding, indicating that young blood rejuvenates, would need to be replicated, ideally at other hospitals, and in more patients, in order to convince researchers. If any benefits stand the test of time, the studies will move on, to tease out the best doses and ages at which to give plasma, how patients’ brains change, and whether improvements make a real difference to the life of someone who can no longer recognize their own family.
Then there is safety. Toying with the ageing process might backfire. Rando is concerned that pumping pro-youthful proteins into people for years could end up giving them cancer. Wyss-Coray agrees it is a worry, but points out that long-term growth hormone therapy appears to be safe. “We just don’t know yet whether or not it will be a problem,” he said.
Rando is more upbeat about infusing patients with pro-youthful proteins for short periods. An elderly person having surgery might get an infusion to help them heal like a teenager. “Let’s say it works. If you can target tissues and improve wound healing in older people, that would be a feasible approach. It would not be about making 90-year-olds younger, or having people live to 150. It’s about healthy living, not longer living,” he said.
In the first human trial of the effects of young blood, at Stanford University, infusions of blood plasma from young people are being given to older people. The preliminary results have surprised the research team, since it appears that all of the cells within the recipients’ bodies are showing marked improvement.
In some countries, there is already a legal market for blood plasma. In the wake of the BSE crisis of the 1990s, plasma donations are not used in the UK. But in the US, donors can make $200 a month (plus loyalty points) from plasma donations. The fresh plasma is separated from the blood, and the red blood cells returned to the bloodstream, in a sitting that lasts 90 minutes. The plasma is used in medical procedures, to treat coagulation disorders and immune deficiencies. The business is completely legitimate, but if young blood rejuvenates our cells is proved to have anti-ageing effects, the risk of backstreet operators setting up will soar. When I asked Wyss-Coray if the prospect worried him, he looked serious. “Absolutely,” he said. “There are always going to be nutcases.”
These are worst-case scenarios. The Stanford trial may find that simply injecting young plasma into old people has little or no effect. Wyss-Coray confesses that he suspects as much. He believes that rejuvenating older people might take a more potent brew than natural plasma. He has in mind a concentrated blend of 10 or 20 pro-youthful factors from young blood, mixed with antibodies that neutralise the effects of ageing factors found in old blood.
“As we get older, we have fewer stem cells and newly born neurons in our brains, and our learning and memory are affected,” says Villeda. “It’s not ddementia it’s just the natural degeneration associated with age.”
Amy Wagers emphasizes that no one has convincingly shown that young blood lengthens lives, and there is no promise that it will. Still, she says that young blood, or factors from it, may hold promise for helping elderly people to heal after surgery, or treating diseases of ageing.
Young mice blood has been studied to cause repair of age related damage such as cardiac hypertrophy, muscle dysfunction, demyelination processes and brain vasculature system in old mice. The mouse is the most common model organism for preclinical studies even though it has not proven particularly reliable at predicting the outcome of studies in humans.
Wyss-Coray one of the authors of the study mentioned in the question is a part of board of directors of a biotechnology start-up named Alkahest to explore the therapeutic implications of the mice findings in humans. The young mice blood treatment has been shown to have effects in old mice neural dysfunctions such as
1. Cardiac hypertrophy: Loffredo et.al. have concluded that treatment of old mice to restore GDF11 to youthful levels recapitulated the effects of parabiosis and reversed age-related hypertrophy, revealing a therapeutic opportunity for cardiac aging in 2013.
2. Muscle dysfunction: GDF11 systemically regulates muscle aging and may be therapeutically useful for reversing age-related skeletal muscle and stem cell dysfunction per conclusions of Sinha M et.al. in 2014.
3. Reversal of demyelination processes: Ruckh JM et.al. in 2012 concluded that enhanced remyelinating (Remyelination is a term for the re-generation of the nerve’s myelin sheath, damaged in many diseases) activity requires both youthful monocytes and other factors, and that remyelination-enhancing therapies targeting endogenous cells can be effective throughout life.
4. Improvement of brain vasculature system: Katsimpardi L et.al. in 2014 concluded that GDF11 alone can improve the cerebral vasculature and enhance neurogenesis. Studies in mice and Xenopus suggest that this protein is involved in mesodermal formation and neurogenesis during embryonic development. Research shows that there could be multiple forms of GDF11
A simple inject-able brain implant is now all it takes to wire up a brain’s neurons. A diverse team of physicists, neuroscientists and chemists has implanted mouse brains with a rolled-up, silky mesh studded with tiny electronic devices, and shown that it unfurls to spy on and stimulate individual neurons.
The inject-able brain implant has the potential to unravel the workings of the mammalian brain in unprecedented detail. “I think it’s great, a very creative new approach to the problem of recording from large number of neurons in the brain,” says Rafael Yuste, director of the Neurotechnology Center at Columbia University in New York, who was not involved in the work.
If eventually shown to be safe, the soft mesh might even be used in humans as an inject-able brain implant to treat conditions such as Parkinson’s disease, concussions and issues arising from Traumatic Brain Injuries, says Charles Lieber, a chemist at Harvard University on Cambridge, Massachusetts, who led the team. The work was published in Nature Nanotechnology on 8 June.
How brain Cells Translate
Neuroscientists still do not understand how the activities of individual brain cells translate to higher cognitive powers such as perception and emotion. The problem has spurred a hunt for technologies that will allow scientists to study thousands, or ideally millions, of neurons at once, but the use of brain implants is currently limited by several disadvantages. So far, even the best technologies have been composed of relatively rigid electronics that act like sandpaper on delicate neurons. They also struggle to track the same neuron over a long period, because individual cells move when an animal breathes or its heart beats.
The Harvard team solved these problems by using a mesh of conductive polymer threads with either nano-scale electrodes or transistors attached at their intersections. Each strand is as soft as silk and as flexible as brain tissue itself. Free space makes up 95% of the mesh, allowing cells to arrange themselves around the inject-able brain implant.
In 2012, the team showed 22 that living cells grown in a dish can be coaxed to grow around these flexible scaffolds and meld with them, but this ‘cyborg’ tissue was created outside a living body. “The problem is, how do you get that into an existing brain?” says Lieber.
The team’s answer was to tightly roll up a 2D mesh a few centimeters wide and then use a needle just 100 micrometers in diameter to inject it directly into a target region through a hole in the top of the skull. The inject-able brain implant mesh unrolls to fill any small cavities and mingles with the tissue (see ‘Bugging the brain’). Nano-wires that poke out can be connected to a computer to take recordings and stimulate cells.
The Injectable Brain Implant
So far, the researchers have utilized the injectable brain implanted meshes consisting of 16 electrical elements into two brain regions of anesthetized mice, where they were able to both monitor and stimulate individual neurons. The mesh integrates tightly with the neural cells, says Jia Liu, a member of the Harvard team, with no signs of an elevated immune response after five weeks. Neurons “look at this polymer network as friendly, like a scaffold”, he says.
The next steps will be to implant larger meshes containing hundreds of devices, with different kinds of sensors, and to record activity in mice that are awake, either by fixing their heads in place, or by developing wireless technologies that would record from neurons as the animals moved freely. The team would also like to inject the device into the brains of newborn mice, where it would unfold further as the brain grew, and to add hairpin-shaped nano-wire probes to the mesh to record electrical activity inside and outside cells.
2014 Conference
When Lieber presented the work at a conference in 2014, it “left a few of us with our jaws dropping”, says Yuste.
There is huge potential for techniques that can study the activity of large numbers of neurons for a long period of time with only minimal damage, says Jens Schouenborg, head of the Neuronano Research Centre at Lund University in Sweden, who has developed a gelatin-based ‘needle’ for delivering electrodes to the brain. But he remains skeptical of this technique: “I would like to see more evidence of the inject-able brain implant’s long-term compatibility with the body,” he says. Rigorous testing would be needed before such a device could be implanted in people. But, says Lieber, it could potentially treat brain damage caused by a stroke, as well as Parkinson’s disease.
Lieber’s team is not funded by the US government’s US$4.5-billion Brain Research through Advancing Innovative Neurotechnologies (BRAIN) initiative, launched in 2013, but the work points to the power of that effort’s multidisciplinary approach, says Yuste, who was an early proponent of the BRAIN initiative. Bringing physical scientists into neuroscience, he says, could help to “break through the major experimental and theoretical challenges that we have to conquer in order to understand how the brain works”.
As a caregiver, we need to be aware of hazards that cause falls, fractures, burns, and other accidents in the home. These incidents cause injury and loss of mobility for individuals who are challenged with vision, balance and coordination impairments. In addition to the pain and expense of the injury, many times depression, social isolation and a feeling of helplessness replace independence.
Some accidents can he caused by medical issues such as sharp drops in blood pressure, numbness in the legs or feet, certain sedatives or anti-depressants, or problems with balance and equilibrium. These problems should be discussed with the individual’s physician as soon as possible. Use this checklist to help make simple changes to make the home safer.
Many accidents can be prevented by thoroughly evaluating the safety of the home and making the necessary modifications. As the old saying goes, “An ounce of prevention is worth a pound of cure”. Take a close look at each entrance, room and stairwell. Check for hazards by using this checklist and then make the needed adaptations to provide a safe environment. By minimizing hazards, you are maximizing independence.
Preventing Falls
Have clutter, newspapers, magazines or other objects been removed from the floor, stairs and counter-tops?
Is there at least one sturdy, easy to grip handrail at the stairway? (Two are recommended if the individuals is utilizing a cane.)
Have all rugs been secured with non-slip pads or tape?
Does the individual wear sturdy, well fitting shoes? (Loose fitting and/or slip-on foot wear can cause an individual to be unstable when walking)
Are there tripping hazards like electrical cords, footstools or other clutter near the floor, which might be difficult to see?
Are lamps and appliances located near the outlets, so extension cords are not needed?
Is the furniture placed with sufficient space allocated for easy egress around the room?
Are the pots, pan and all the cooking utensils placed at a comfortable height?
Is there a “Reaching Devise” available to utilize when selecting difficult to reach items in cabinets and on shelves?
If a stepladder must be used, is it sturdy with handles and textured steps?
Is there a sturdy cane, crutch, walker or bar close to the bed and chairs to assist in getting up?
Can personal items such as eyeglasses, tissues, TV remotes or telephones easily be reached while in bed or sitting in a chair?
Are light switches easily accessible?
Have you considered changing the standard toggle switch to a rocker switch to help with ease of operating?
Is the toilet at a comfortable height? (Consider adding a raised toilet seat, a toilet safety frame with armrests, or an over toilet adjustable commode)
Are there grab bars near the toilet and tub and/or shower area? TOWEL BARS SHOULD NEVER BE USED AS HANDRAILS.
Is there a bath chair in the shower area?
Does the individual need a transfer tub bench to get in or out of the bathtub?
Is there a hand-held shower spray that can be used while sitting on a bath chair or bench?
Are necessary bath items (towels, washcloths, soap, shampoo, etc.) stored in an easy to reach location?
Are towel bars, toilet and sink fixtures securely attached?
Does the bathtub and/or shower have a non-slip surface?
Are the knobs in the sink and tub clearly labeled. as hot and cold?
(If necessary, mark the hot water knob with red nail polish as a
reminder.)
Are the thermostat, electrical outlets and light switches at easily reached heights?
Are outdoor steps kept sturdy and textured to prevent slipping? (Add tread strips to provide texture)
Lighting
Adequate lighting is essential throughout the home for safety and ‘Ay of life As individuals grow older, vision diminishes because …eyes restrict the amount of light that is coming in and is being absorbed. Frustration is common as simple tasks become more fi(&t because of vision changes. Make sure that regular eye exams j eyeglass prescriptions are kept up to date You can also help by making some modifications within the home.
Is the lighting uniform from one room to the other? (Older eyes t ‘ke longer to adjust to light levels)
Have you increased natural lighting by checking to see if windows and screens are clean?
Is the lighting glare free? (eyes become more sensitive to glare as they age)
Are all rooms hallways stairwells and entrances well lit?
Are night -lights used in the bedrooms and bathrooms? (Motion activated lights do not interfere with sleeping.)
Is there a motion activated light at the entranceway?
If the threshold is at a different level it is adequately lit?
Is lighting adequate for reading, sewing hobbies etc”
Are there light switches at the top and bottom of staircases?
Is there a plug-in rechargeable flashlight near each bed?
Have wattages of bulbs been increased in lamps and fixtures to compensate for loss of vision? (Caution do not exceed ‘ianufactures posted guidelines)
Other Safety Concerns
Everyday safety practices and emergency planning cannot be left to chance. Review the plans with the individual periodically and practice emergency evacuations.
Are emergency phone numbers AND the address of the residence posted near each telephone?
Has everyone in the home been taught how to call 9-1-11 ● Is there an escape plan in case of fire?
Is there a tornado or “shelterin place’ plan of action in place? ● Have all cords and wires been checked for fraying or wear?
Is there a fire extinguisher readily available?
Are smoke alarms and carbon monoxide alarms installed near each bedroom and the kitchen?
Are batteries checked and changed when needed in smoke and carbon monoxide alarms monthly? Have non-working alarms been replaced?
Are outlets and plugs warm? If so, avoid using until an electrician can check them.
Are electrical outlets overloaded with cords? (Never have more
than one high-wattage appliance plugged into a single outlet.)
Avoid space heaters if possible. If they must be used, make sure
that they are kept away from flammable materials.
Is water temperature set at 120 degrees or less to prevent burns?
Are flammable liquids stored away from heat sources?
Are hot and cold-water knobs marked clearly? (Label the hot water knob with nail polish or paint, if necessary.)
Can doorknobs be opened by the individual? (Consider changing knobs to levers that are easier to open.)
Can the individual lock and unlock the door?
This guide nformation originated from the United Cerebral Palsy of Greater Birmingham
Does DeepMind represent the initial step in software development becoming a major assist or replacement for controlling bodily functions in individual with Traumatic Brain and/or Spinal Cord injuries? Imagine a person suffering from one of those afflictions utilizing software to control the muscle functions of their body as they go about their normal everyday activities.
DeepMind, the Google-owned artificial-intelligence company, has revealed how it created a single computer algorithm that can learn how to play 49 different arcade games, including the 1970’s classics Pong and Space Invaders. In more than half of those games, the computer became skilled enough to beat a professional human player.
The algorithm — which has generated a buzz since publication of a preliminary version in 2013 (V. Mnih et al. Preprint at http://arxiv.org/abs/1312.5602; 2013) — is the first artificial-intelligence (AI) system that can learn a variety of tasks from scratch given only the same, minimal starting information. “The fact that you have one system that can learn several games, without any tweaking from game to game, is surprising and pretty impressive,” says Nathan Sprague, a machine-learning scientist at James Madison University in Harrisonburg, Virginia.
DeepMind, which is based in London, says that the brain-inspired system could also provide insights into human intelligence. “Neuroscientists are studying intelligence and decision-making, and here’s a very clean test bed for those ideas,” says Demis Hassabis, co-founder of DeepMind. He and his colleagues describe the gaming algorithm in a paper published this week
Games are to AI researchers what fruit flies are to biology — a stripped-back system in which to test theories, says Richard Sutton, a computer scientist who studies reinforcement learning at the University of Alberta in Edmonton, Canada. “Understanding the mind is an incredibly difficult problem, but games allow you to break it down into parts that you can study,” he says. But so far, most human-beating computers — such as IBM’s Deep Blue, which beat chess world champion Garry Kasparov in 1997, and the recently unveiled algorithm that plays Texas Hold ’Em poker essentially perfectly.
DeepMind’s versatility comes from joining two types of machine learning— an achievement that Sutton calls “a big deal”. The first, called deep learning, uses a brain-inspired architecture in which connections between layers of simulated neurons are strengthened on the basis of experience. Deep-learning systems can then draw complex information from reams of unstructured data (seeNature505, 146–148; 2014). Google, of Mountain View, California, uses such algorithms to automatically classify photographs and aims to use them for machine translation.
The second is reinforcement learning, a decision-making system inspired by the neurotransmitter dopamine reward system in the animal brain. Using only the screen’s pixels and game score as input, the algorithm learned by trial and error which actions — such as go left, go right or fire — to take at any given time to bring the greatest rewards. After spending several hours on each game, it mastered a range of arcade classics, including car racing, boxing and Space Invaders.
This rapid growth of data sets means that machine learning can now use complex model classes and tackle highly non-trivial inference problems. Our human brain constantly solves non-trivial problems as we conduct our daily activities. Interpreting high-dimensional sensory data to determine how best to control all of the muscles in our body, including the functioning of our internal organs. The development of cutting edge software, like DeepMind, could assist and resolve many of the issues confronting Traumatic Brain and Spinal Cord Injury patients, beginning with recovering the ability to move their arms and legs.
Following a car crash, Mr. Constantine had a traumatic brain stem stroke that caused paralysis on the right side of his body. His leg muscles became so severely spastic that he could not walk. After four years of confinement to a wheelchair, Rick Constantine, 58, is now walking again after undergoing an unconventional surgery at University of California, San Diego Heath System to restore the use of his leg. Neurosurgeon Justin Brown, MD, director of the Neurosurgery Peripheral Nerve Program at UC San Diego Health System, performed the novel 3-hour procedure. His team performed a delicate surgery to reduce input from the nerves that were causing the muscles to over contract to the point of disability.
“After my injury, I was told I would never walk again. All I could to was move from my wheelchair to my bed or a chair,” said Constantine, a former NASCAR crew member. “After surgery with Dr. Brown, I could put my foot flat on the ground to walk. With physical therapy, everything just gets better and better. I’m a firm believer in never giving up.”
Prior to surgery, Constantine underwent botox treatments and physical therapy in an attempt to restore the use of his leg following the injury due to his traumatic brain stem stroke. The results were positive but minimal. An additional nerve conduction study, called an electromyogram (EMG), identified the muscles causing the dysfunction.
“When all other options did not produce satisfying results, we opted for surgery,” said Brown. “With the EMG, we identified the over excited nerves resulting from the traumatic brain stem stroke, which needed to be downgraded. Mr. Constantine had surgery on a Friday and within days was in physical rehabilitation. Two weeks later he was walking without a walker and has even completed a 1-mile race without assistance.”
The surgery, called a selective peripheral neurotomy, is a procedure performed under a microscope. Brown makes an incision behind the knee to reach the tibial nerve. He then selectively trims back the troublesome nerve branches by up to 80 percent. Cutting the nerve reduces the “noise” being relayed back to the spinal cord which causes the spasticity.
Brown, who also serves as co-director of the Center for Neurophysiology and Restorative Neurology at UC San Diego Health System, said the advantage to this approach is that the muscle is preserved and there is no need to cut or lengthen the tendon.
Depending on the specific patient and their medical history, selective peripheral neurotomy may be appropriate for patients with brain and spinal cord injury from strokes or tumors, cerebral palsy, or multiple sclerosis.
No special post-operative care is required as the sutures are absorb-able. Rehabilitation can begin 72 hours after the procedure and Constantine underwent physical therapy at VIP Neuro-Rehabilitation Center in San Diego.
Dr. Justin Brown has performed this surgery on six patients, which is seldom performed in the United States, but more common in France and Japan.
A Spinal Cord rehab breakthrough occurred at the University of Louisville Spinal Cord research lab , when neuroscientist Susan Harkema turned her back to her study subject to check a reading on a computer screen.
“Hey Susie, look at this,” the patient called out to her. “I can move my toe!“
It’s not the first time electrical stimulation has made paralyzed patients move, but Harkema says it’s the first time electrical stimulation directly to the spinal cord has shown voluntary activity. Experts say this new technique is another piece of the puzzle toward helping paralyzed people walk again. And it’s another avenue doctors can go down to try to help these patients.
“This is a breakthrough,” says Dr. Barth Green, co-founder of The Miami Project to Cure Paralysis at the University of Miami, who was not involved in the research. “It shows you can have a living spinal cord under the layer of their injury.”
More than 1,700 paralyzed people have inquired about using this technology, which involves surgically implanting a stimulator and giving it directions with an external remote control. The stimulator creates a small, slightly visible bulge in the lower abdomen and is connected to wires that send electrical pulses to the spinal cord.
But patients shouldn’t expect that the stimulator will help them walk, since the stimulator can only make one leg work at a time. Patients have to turn the stimulator off and then back on again to make the other leg work or to make another set of muscles such as their torsos work.
Even though Dustin Shillcox, the fourth patient to try the device, can’t walk, the stimulator has had other benefits dramatically improving bladder, bowel and sexual function amazingly changing his entire life.
Plus, tests showed the patients, who could finally move their legs and torsos after years of paralysis, became healthier in general with improved heart and respiratory function.
“If you can change health and wellness and life expectancy, to me that’s a home run,” Green says. “Remember, Christopher Reeve died from complications of immobility,”
The researchers are pretty much stumped as to exactly why electrical stimulation to the spinal cord created the movement on demand — after all, they didn’t touch the patients’ brains. Perhaps, Harkema says, the spinal cord in a way has a brain of its own. “Maybe the spinal cord makes the decision to move on its own and then executes the movement,” Harkema says. “Otherwise I don’t know how you would see what we see today.”
The Louisville researchers now have funding to implant the device in eight more patients. They hope a device company will help them come up with a way to stimulate more than one muscle group at the time.
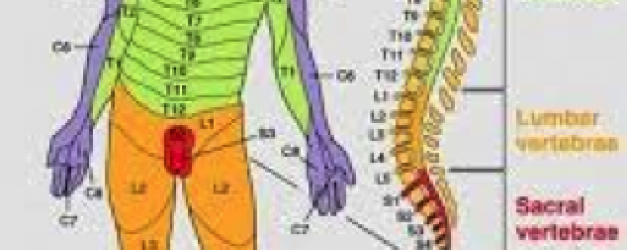
Traumatic Brain or Spinal Cord Injury can result in damaging neurons in the brain or spinal cord. When communication between the brain and spinal cord fails, paralysis occurs affecting only the areas below the level of injury.
Messages are passed from neuron to neuron through small gaps between the cells, with the help of chemicals called neurotransmitters. To transmit an action potential message neurotransmitter molecules are released from one neuron across the gap to the next neuron this process continues until the message reaches its destination.There are millions and millions of connections between neurons within the spinal cord alone which connections are made during our body’s development.
NEUROTRANSMITTERSare the brain chemicals that communicate information throughout our brain and body. They relay signals between nerve cells, called “neurons.” The brain uses neurotransmitters to tell your heart to beat, your lungs to breathe, and your stomach to digest. They can also affect mood, sleep, concentration, weight, and can cause adverse symptoms when they are out of balance. Neurotransmitter levels can be depleted many ways – from stress, poor diet, neurotoxins, genetic predisposition, drugs , alcohol and caffeine usage.
There are two kinds of neurotransmitters – INHIBITORY and EXCITATORY. Excitatory neurotransmitters are not necessarily exciting – they are what stimulate the brain. Those that calm the brain and help create balance are called inhibitory. Inhibitory neurotransmitters balance mood and are easily depleted when the excitatory neurotransmitters are overactive.
SEROTONIN is an inhibitory neurotransmitter – which means that it does not stimulate the brain. Adequate amounts of serotonin are necessary for a stable mood and to balance any excessive excitatory (stimulating) neurotransmitter firing in the brain. If you use stimulant medications or caffeine in your daily regimen – it can cause a depletion of serotonin over time. Serotonin also regulates many other processes such as carbohydrate cravings, sleep cycle, pain control and appropriate digestion. Low serotonin levels are also associated with decreased immune system function.
GABA is an inhibitory neurotransmitter that is often referred to as “nature’s VALIUM-like substance”. When GABA is out of range (high or low excretion values), it is likely that an excitatory neurotransmitter is firing too often in the brain. GABA will be sent out to attempt to balance this stimulating over-firing.
DOPAMINE is a special neurotransmitter because it is considered to be both excitatory and inhibitory. Dopamine helps with depression as well as focus, which you will read about in the excitatory section.
DOPAMINE is our main focus neurotransmitter. When dopamine is either elevated or low – we can have focus issues such as not remembering where we put our keys, forgetting what a paragraph said when we just finished reading it or simply daydreaming and not being able to stay on task. Dopamine is also responsible for our drive or desire to get things done – or motivation. Stimulants such as medications for ADD/ADHD and caffeine cause dopamine to be pushed into the synapse so that focus is improved. Unfortunately, stimulating dopamine consistently can cause a depletion of dopamine over time.
NOR-EPINEPHRINE is an excitatory neurotransmitter that is responsible for our stimulation processes in the body. Norepinephrine helps to make epinephrine as well. This neurotransmitter can cause ANXIETY at elevated excretion levels as well as some “MOOD DAMPENING” effects. Low levels of norepinephrine are associated with LOW ENERGY, DECREASED FOCUS ability and sleep cycle problems.
EPINEPHRINE is an excitatory neurotransmitter that is reflective of stress. This neurotransmitter will often be elevated when ADHD like symptoms are present. Long term STRESS or INSOMNIA can cause epinephrine levels to be depleted (low). Epinephrine also regulates HEART RATE and BLOOD PRESSURE.
This new development utilizing an Optical Brain Scanner may revolutionize the future treatment of Traumatic Brain Injury patients due to its portability and non-invasive technology. With further refinement and development, these features will allow EMT’s to do a comprehensive evaluation on the patient prior to transporting them to the hospital and share the imaging data with neurologists.
Scientists have advanced a brain-scanning technology that tracks what the brain is doing by shining dozens of tiny LED lights on the head. This new generation of neuroimaging compares favorably to other approaches but avoids the radiation exposure and bulky magnets the others require, according to new research at Washington University School of Medicine in St. Louis.
The new optical approach to brain scanning is ideally suited for children and for patients with electronic implants, such as pacemakers, cochlear implants and deep brain simulators (used to treat Parkinson’s disease). The magnetic fields in magnetic resonance imaging (MRI) often disrupt either the function or safety of implanted electrical devices, whereas there is no interference with the optical technique.
The new technology is called diffuse optical tomography (DOT). While researchers have been developing it for more than 10 years, the method had been limited to small regions of the brain. The new DOT instrument covers two-thirds of the head and for the first time can image brain processes taking place in multiple regions and brain networks such as those involved in language processing and self-reflection (daydreaming).
“When the neuronal activity of a region in the brain increases, highly oxygenated blood flows to the parts of the brain doing more work, and we can detect that,” said senior author Joseph Culver, PhD, associate professor of radiology. “It’s roughly akin to spotting the rush of blood to someone’s cheeks when they blush.”
The technique works by detecting light transmitted through the head and capturing the dynamic changes in color of the brain tissue.
Although DOT technology now is used in research settings, it has the potential to be helpful in many medical scenarios as a surrogate for functional MRI, the most commonly used imaging method for mapping human brain function. Functional MRI also tracks activity in the brain via changes in blood flow. In addition to greatly adding to our understanding of the human brain, fMRI is used to diagnose and monitor brain disease and therapy.
Another commonly used method for mapping brain function is positron emission tomography (PET), which involves radiation exposure. Because DOT technology does not use radiation, multiple scans performed over time could be used to monitor the progress of patients treated for brain injuries, developmental disorders such as autism, neurodegenerative disorders such as Parkinson’s, and other diseases.
Unlike fMRI and PET, DOT technology is designed to be portable, so it could be used at a patient’s beside, in the operating room.or at point of injury as in the case of Traumatic Brain Injuries and concussions.
“With the new improvements in image quality, DOT is moving significantly closer to the resolution and positional accuracy of fMRI,” said first author Adam T. Eggebrecht, PhD, a postdoctoral research fellow. “That means DOT can be used as a stronger surrogate in situations where fMRI cannot be used.”
For the current study, the researchers validated the performance of DOT by comparing its results to fMRI scans. Data was collected using the same subjects, and the DOT and fMRI images were aligned. They looked for Broca’s area, a key area of the frontal lobe used for language and speech production. The overlap between the brain region identified as Broca’s area by DOT data and by fMRI scans was about 75 percent.
“With the improved image quality of the new DOT system, we are getting much closer to the accuracy of fMRI,” Culver said. “We’ve achieved a level of detail that, going forward, could make optical neuroimaging much more useful in research and the clinic.”
While DOT doesn’t let scientists peer very deeply into the brain, researchers can get reliable data to a depth of about one centimeter of tissue. That centimeter contains some of the brain’s most important and interesting areas with many higher brain functions, such as memory, language and self-awareness represented.
During DOT scans, the subject wears a cap composed of many light sources and sensors connected to cables. The full-scale DOT unit takes up an area slightly larger than an old-fashioned phone booth, but Culver and his colleagues have built versions of the scanner mounted on wheeled carts. They continue to work to make the technology more portable.
The research is funded by the National Institutes of Health (NIH) grants R01-EB009233, R01-NS078223, T32-NS007205-30 and P30-NS048056; an Autism Speaks Postdoctoral Translational Research Fellowship; a Fulbright Science and Technology PhD Award; and a McDonnell Centre for Systems Neuroscience grant.

 I recently visited The Red Barn meeting with the founder, Joy O’Neal, who spent the greater part of the day touring me through the facility while explaining the unique approach of equestrian therapy. Individuals in need of therapeutic intervention are often difficult to reach through the standard therapy programs available. The Red Barn has developed an equestrian therapy intervention program that breaks down those self imposed barriers. Here working one on one with a patient assisted by horses, allows them to introduce a series of training courses focused on improving their overall well being.
I recently visited The Red Barn meeting with the founder, Joy O’Neal, who spent the greater part of the day touring me through the facility while explaining the unique approach of equestrian therapy. Individuals in need of therapeutic intervention are often difficult to reach through the standard therapy programs available. The Red Barn has developed an equestrian therapy intervention program that breaks down those self imposed barriers. Here working one on one with a patient assisted by horses, allows them to introduce a series of training courses focused on improving their overall well being.